OCT Risk Factors for Geographic Atrophy Progression
 Jeong W. Pak, Thomas Saunders, Rick Voland, Barbara A. Blodi, Amitha Domalpally
Jeong W. Pak, Thomas Saunders, Rick Voland, Barbara A. Blodi, Amitha Domalpally
Abstract
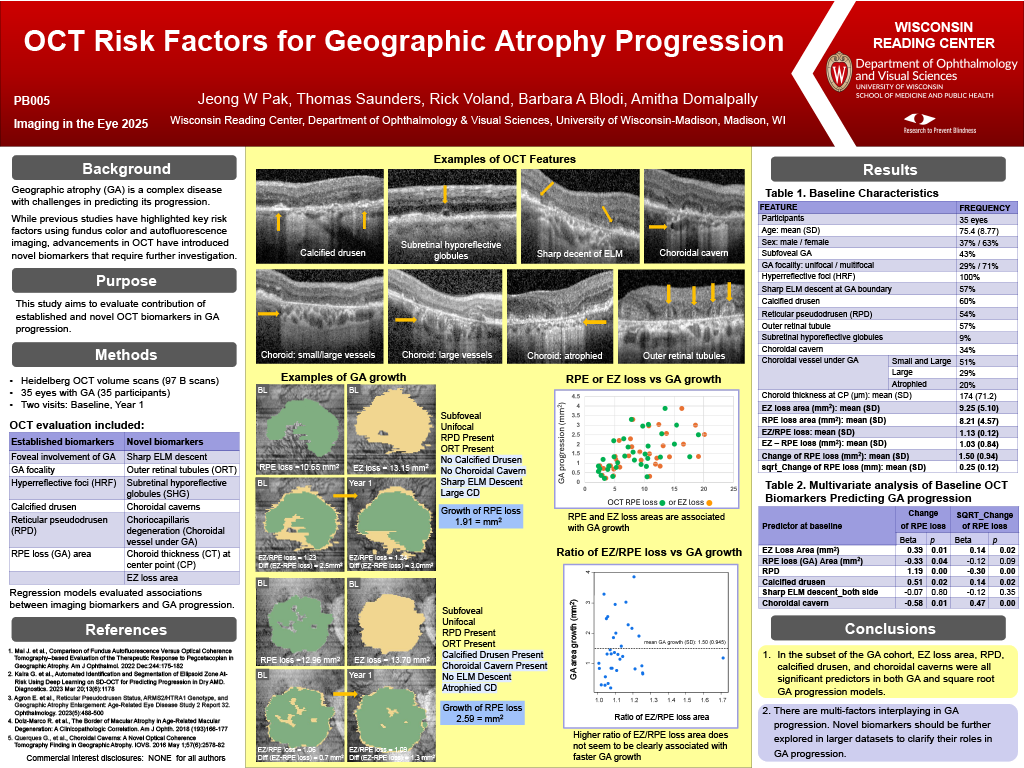
Purpose: Geographic atrophy (GA) is a complex disease with challenges in predicting its progression. While previous studies have highlighted key risk factors using fundus color and autofluorescence imaging, advancements in OCT have introduced novel biomarkers that require further investigation. This study aims to identify novel OCT biomarkers contributing to GA progression.
Methods: Heidelberg OCT of 35 eyes (35 participants) with two visits one year apart were analyzed. OCT evaluation included foveal involvement, focality, reticular pseudodrusen (RPD), calcified drusen, outer retinal tubules (ORT), sharp ELM descent, choroid thickness (CT) at center point, choriocapillaris degeneration, choroidal caverns, subretinal hyporeflective globules (SHG), ellipsoid zone (EZ) loss area, retinal pigment epithelium (RPE) loss area, EZ/RPE loss ratio, and EZ loss minus RPE loss. Regression models evaluated associations between OCT biomarkers and GA (RPE loss) progression.
Results: Mean (SD) baseline (BL) GA area was 8.21 mm2 (4.57) with a mean rate of progression of 1.50 mm2 (0.94). GA was subfoveal in 43% of eyes and multifocal in 71%. RPD was present in 54%, calcified drusen in 60%, ORT in 57%, ELM descent in 57%, atrophied choroidal vessels under GA in 20%, choroidal caverns in 34%, and SHG in 9%. Mean CT was 174 (71.2) µm. Mean EZ loss area was 9.25 mm2 (5.10), mean EZ/RPE ratio was 1.13 mm2 (0.12), and the mean area difference between EZ loss and RPE loss was 1.03 mm2 (0.84). Univariate regression analyses identified GA multifocal, calcified drusen, choroidal caverns, SHG, BL EZ loss area, BL GA area, and the mean area difference between EZ loss and RPE loss as significant predictors of GA progression. Multivariate regression, adjusted for covariates with p <0.05 in univariate models, revealed BL calcified drusen and SHG as significant predictors. EZ loss area remained significant in one model, while the difference between EZ loss and RPE loss was not independently associated.
Conclusions: In the subset of the GA cohort, calcified drusen, choroidal caverns, and SHG were all significant predictors in both GA and square root GA progression models. Multifocal GA was significant only in square root GA progression model, while EZ loss area, RPE loss area, and the area difference between EZ loss and RPE loss were significant only in GA progression model. Novel biomarkers should be further explored in larger datasets to clarify their roles in GA progression.