Real World Deployment of a Prescreening Algorithm for Geographic Atrophy
Thomas Saunders, Robert Slater, Roomasa Channa, Barbara A. Blodi, Amitha Domalpally
Abstract
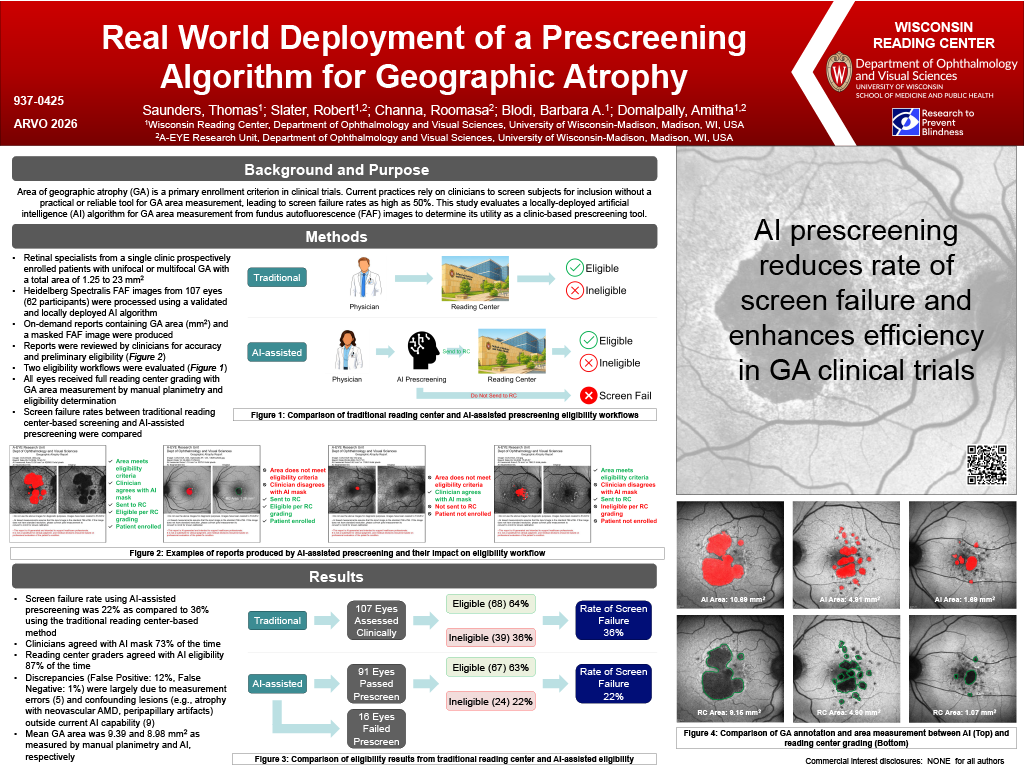
Purpose: Area of geographic atrophy (GA) is a primary enrollment criterion in clinical trials. Current practices rely on clinicians to screen subjects for inclusion without a practical or reliable tool for GA area measurement, leading to screen failure rates as high as 50%. This study evaluates a locally deployed artificial intelligence (Al) algorithm for GA area measurement from fundus autofluorescence (FAF) images to determine its utility as a clinic-based prescreening tool.
Methods: Retina specialists from a single clinic were asked to prospectively enroll patients with unifocal or multifocal GA with a total area of 1.25 to 23 mm2, with at least 70% between 2.5 and 17.5 mm2. Heidelberg Spectralis FAF images were processed using a validated and locally deployed Al algorithm, producing an immediate report with both measurement of GA area (mm2) and a masked FAF image indicating GA lesions, allowing clinicians to visually verify what the model measured. Reports were reviewed by clinicians for accuracy and preliminary eligibility before submitting images to the reading center for final determination. All cases, including those deemed ineligible or with inaccurate reports, were included for review by the reading center. Screen failure rates between Al-assisted prescreening and traditional reading center-based screening were compared.
Results: Clinicians submitted 107 eyes from 62 participants. Al-assisted prescreening identified 80 eyes as eligible and 27 as ineligible. Reading Center confirmed eligibility in 67 of the 80 prescreened eligible eyes. Of the 27 determined ineligible by Al-assisted prescreening, 1 was confirmed eligible by the reading center. Mean GA area was 9.39 and 8.98 mm2 as measured by manual planimetry and Al, respectively. Discrepancies (False Positive: 12%, False Negative: 1%) were largely due to measurement errors (5) and confounding lesions (e.g. atrophy with neovascular AMO, peripapillary artifacts) outside current Al capability (9). Screen failure rate using Al-assisted prescreening was 16% as compared to 25% using the traditional reading center-based method.
Conclusions: A significant reduction in screen failure rate coupled with good sensitivity and specificity suggests that Al-assisted prescreening may be beneficial in GA clinical trials. Integration into standard practice has the potential to improve efficiency and accuracy at the clinic level and decrease burden on sites and trial participants.