A Comparison of Neovascular Age-Related Macular Degeneration Features in OCT Angiography and Fluorescein Angiography (2013)
 Jordan Winkler, Rachel Linderman, Jeong Pak, Mary Wilda, Rick Voland, Amitha Domalpally, Barbara Blodi
Jordan Winkler, Rachel Linderman, Jeong Pak, Mary Wilda, Rick Voland, Amitha Domalpally, Barbara Blodi
Abstract
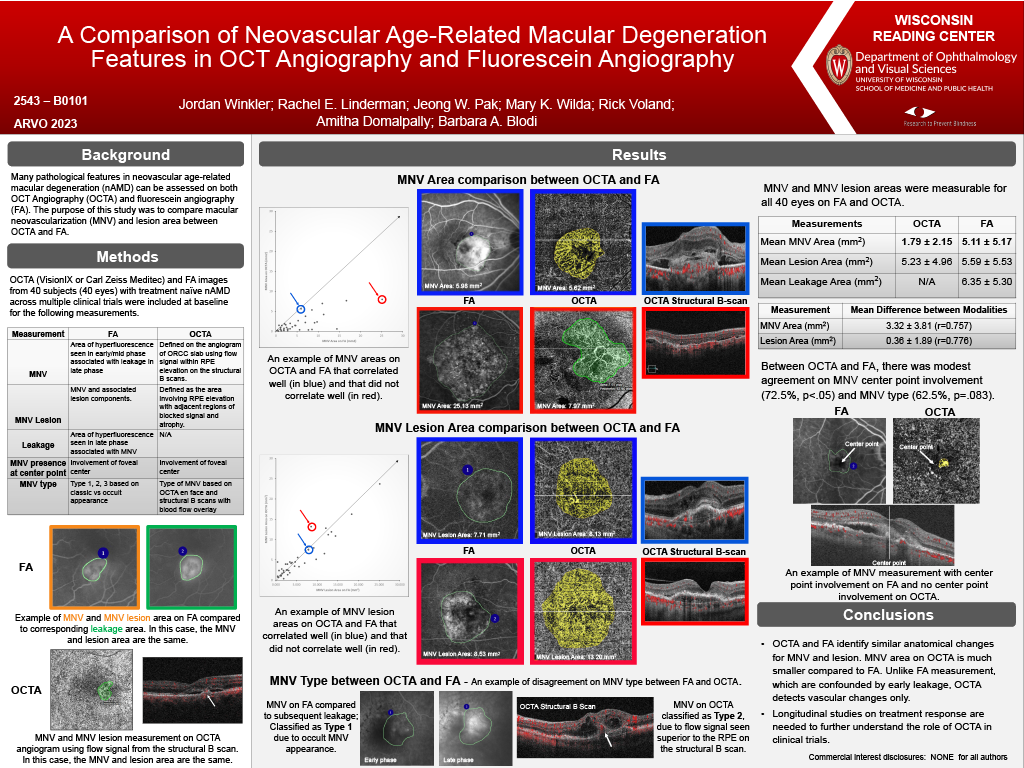
Purpose: Numerous pathological features in neovascular age-related macular degeneration (nAMD) can be assessed on both OCT-Angiography (OCTA) and fluorescein angiography (FA). We sought to compare macular neovascularization (MNV) and lesion area between OCTA and FA.
Methods: OCTA and FA images from 30 subjects with treatment naïve nAMD across multiple clinical trials were included at baseline. MNV area (mm¬2), lesion area within ETDRS grid (mm2), MNV type, and MNV presence at center point were evaluated from OCTA (VisionIX or Carl Zeiss Meditec) and FA while total leakage area within the ETDRS grid (mm2) was assessed only on FA. For OCTA, MNV area was defined on the angiogram using the flow signal within RPE elevation on the cross-sectional scan. OCTA lesion area was defined as the area involving RPE elevation with adjacent regions of blocked signal and atrophy. MNV from FA was identified by area of hyperfluorescence seen in early/mid phase associated with leakage in late phase. FA lesion area was defined by the MNV and associated lesion components. Comparisons of features assessed on OCTA versus FA were performed.
Results: MNV was measurable for 28 of 30 subjects on OCTA, while all subjects had visible MNV on FA. All subjects had assessable lesion area on OCTA and FA. Mean MNV area and lesion area on OCTA were 1.91 ± 2.17 mm2 and 5.45 ± 5.77 mm2. With FA, the measurements were 4.86 ± 5.44 mm2 and 5.43 ± 5.91 mm2 respectively. Mean difference between the two modalities was 2.95 ± 3.70 mm2 (r = 0.91) for MNV area and 0.03 ± 0.053 mm2 (r = 0.99) for lesion area. Leakage area on FA was also correlated with both MNV area and lesion area on OCTA (r = 0.886 and r = 0.942 respectively). When visually comparing measurements between FA and OCTA, lesions were measured at similar locations on both imaging types (Figure 1, A-B) but the general shape of the lesions could vary (Figure 1, C-D). There was modest agreement on center point involvement of MNV between OCTA and FA at 71.4% (p < 0.05); The agreement on the type of MNV lesions was poor between OCTA and FA with 44% agreement (p = 0.40).
Conclusion: While OCTA and FA appear to identify similar presence of both MNV and the associated lesion, there was a significant difference in the MNV area measurements between the two modalities. Longitudinal studies on treatment response are needed to further understand the role of FA and OCTA in clinical trials.